Why leisure contacts must be reduced
Belgium’s Consultative Committee took drastic measures on Friday, October 16 as a result of the epidemiological situation and the burden on the health system by further limiting close contacts, imposing teleworking where possible and enforcing the closure of pubs and restaurants for a period of at least four weeks (with a re-evaluation of the situation after two weeks). Unfortunately, reducing the number of contacts, especially during leisure time, is a necessary step in order to reduce the transmission of the virus and to lower the risk of new stringent measures such as a lockdown including school closure, closure of borders and a standstill of all economic activities, through closure of non-essential businesses, to a large extent.
The intervention measures taken are focusing on the reduction of contacts made during our social lives and more specifically in restaurants and bars. Evidence exists from international scientific literature that COVID-19 outbreaks are linked to social venues (1). However, in Belgium, there is a lot of uncertainty about the exact setting in which SARS-CoV-2 transmission occurs, especially since detailed whereabouts (i.e., including the possible source of infection) concerning confirmed cases are lacking to date. Consequently, there is no conclusive Belgian evidence that these places constitute hotspots of disease transmission nor that these places are the single location at which transmission occurs. Needless to say, these specific measures are closely linked to the ones targeting a reduction in social contacts (i.e., having a single close contact during this period). As we want to safeguard our school and healthcare system, a reduction in leisure time contacts is of the utmost importance.
In order to show the extent of the interventions on the spread of the disease, the potential impact thereof is quantified in terms of a relative increase or decrease in the number of contacts depending on the location at which those are made. More specifically, physical person-to-person contacts are classified in different categories such as family contacts, work contacts, school contacts, leisure contacts, etc. These contact rates are estimated from so-called social contact surveys, either in pre-pandemic times or during the pandemic (see, e.g., Belgian CoMix data, Coletti et al., 2020) and adapted with an estimation of the reduction of transmission through sanitary measures like keeping distance and mask wearing. This information naturally fits into a mathematical modelling approach that describes the disease spread in the Belgian population.
From the initial lockdown period in March, the relative contributions of these location-specific contacts to the total number of age-dependent and effective contacts enabling SARS-CoV-2 transmission have been estimated using mathematical models, in combination with the probability of transmission. Hence, these models allow to study scenarios analysis with a comparison of different approaches to partial restriction of contacts in a specific category.
Scenario analyses for hospital load and incidence of new hospitalizations
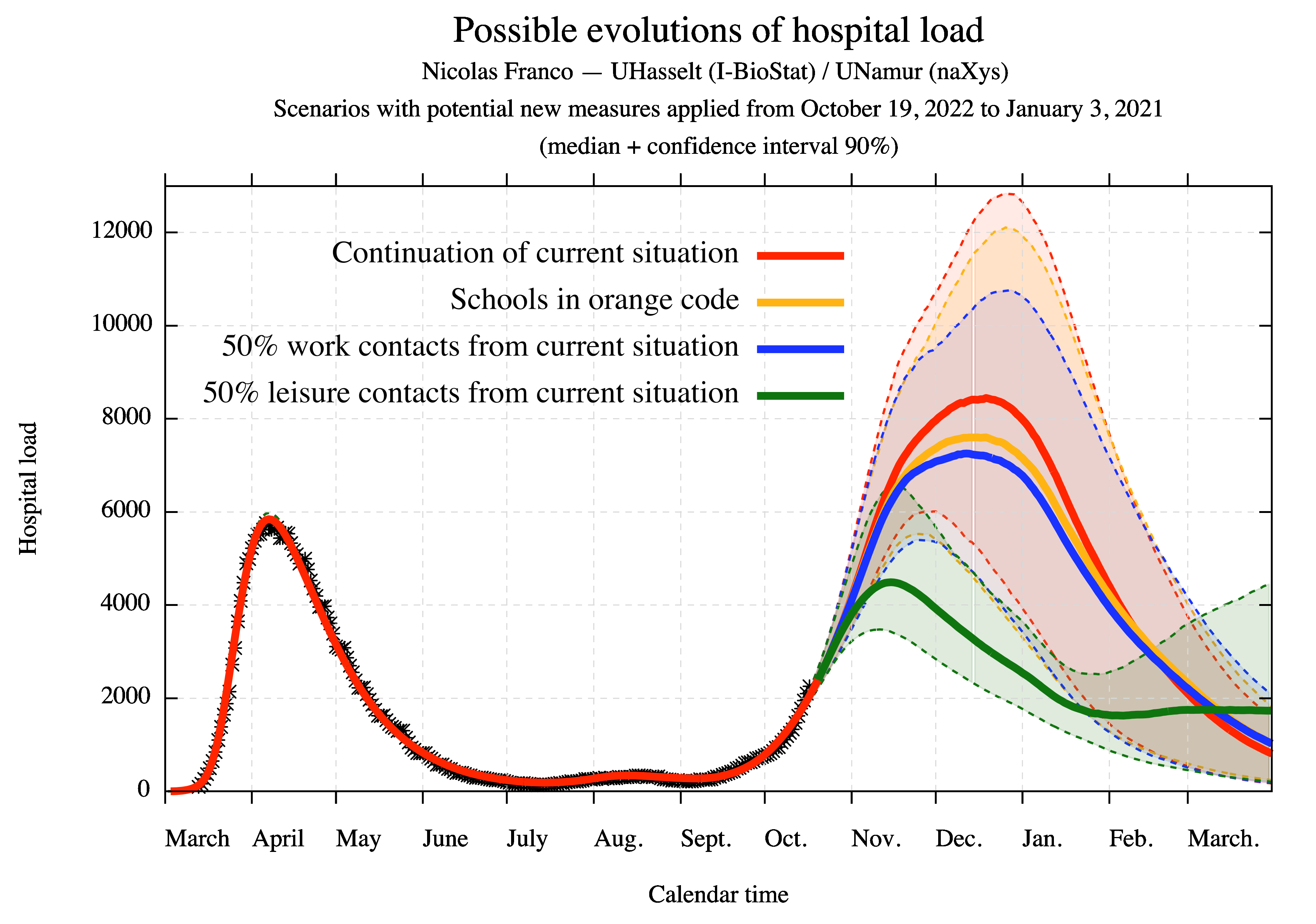
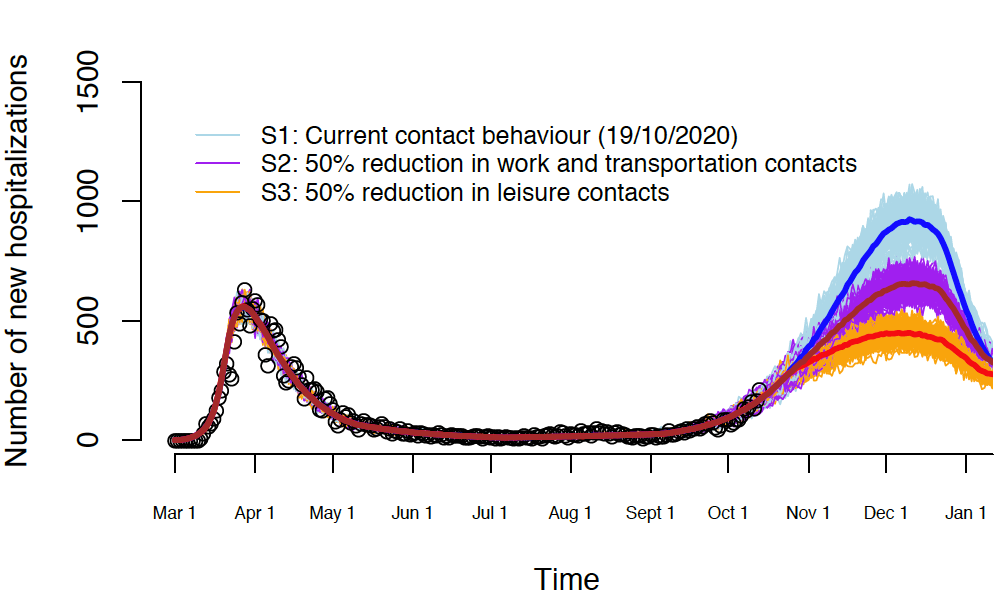
Our model predictions of the epidemic from mid-October onwards, based on the methods described in Franco (2020) and Abrams et al. (2020), are problematic as they indicate the risk of an overload of hospital capacities during a long period of high incidence, associated with increased hospital admissions between November and January. These models can predict the potential impact of the reduction of school contacts at the level of the defined “code orange”, but we found that this effect is minimal and does not avoid an overload problem. The potential impact of mandatory telework is more pronounced, but insufficient on its own.
A reduction of 50% of the contacts occurring during leisure time drastically decreases the peak size of the upcoming second wave in terms of hospital load and daily incidence of hospitalizations after only 2 to 3 weeks. Here, leisure contacts refer to social contacts that do not take place at home, work, transport and school. Note that “continuation of the current situation” refers to the situation prior to the most recent interventions (started on October 19, 2020) and is based on the best model fits until 18/10.
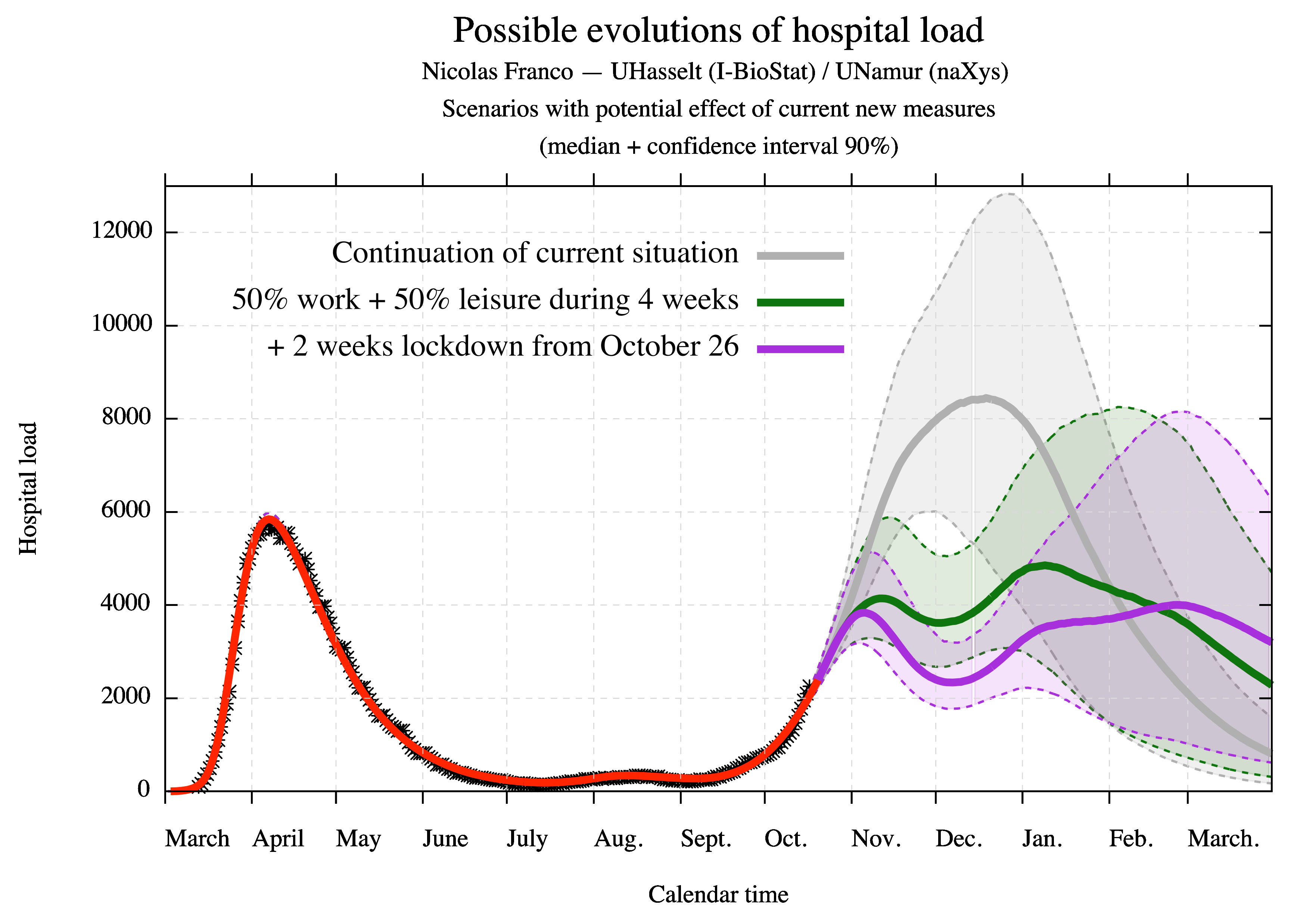
Will the new efforts be enough to hammer the new wave?
This will, most importantly, depend on the overalls people’s behaviour, during the following four-week period and afterwards. Four weeks is sufficiently long to stop the current increase in new hospitalizations as long the new and established measures are respected (including the 6 golden rules 2). However, these efforts on their own might not be sufficient to prevent a resurgence or restart of the increase in December, or later on, if contact behaviour is re-instated. It is most likely that continued endeavours are required during 2021 in order to keep virus circulation low enough to allow functional test and trace strategies, to keep our schools open to the maximum, to protect the most vulnerable individuals in our society, to avoid again more stringent measures and associated mental health problems, and to prevent our healthcare system from collapsing.
References:
- Coletti, P., Wambua, J., Gimma, A., Willem, L., Vercruysse, S., Vanhoutte, B., Jarvis, C. I., van Zandvoort, K., Edmunds, J., Beutels, P., Hens, N. (2020). CoMix: comparing mixing patterns in the Belgian population during and after lockdown. medRxiv.
- Franco, N. (2020). Covid-19 Belgium: Extended SEIR-QD model with nursery homes and long-term scenarios-based forecasts from school opening. medRxiv.
- Abrams, S., Wambua, J., Santermans, E., Willem, L., Kuylen, E., Coletti, P., Libin, P., Faes, C., Petrof, O., Herzog, S. A., The SIMID COVID-19 team, Beutels, P., Hens, N. (2020). Modeling the early phase of the Belgian COVID-19 epidemic using a stochastic compartmental model and studying its implied future trajectories. medRxiv.
See also:
- https://www.cdc.gov/mmwr/volumes/69/wr/mm6936a5.htm
- https://www.info-coronavirus.be